Antibody-drug conjugates (ADCs) are becoming an exciting part of the treatment landscape for breast and ovarian cancer patients. Recent studies have shown particular success in ADC designs targeting HER2, TROP2, FRα, and NaPi2b to precision-deliver cytotoxic drugs directly to the tumor cells by exploiting the overexpression of these antigens on cancer cells compared to healthy tissue.(1,2)
The key components of an ADC include a tumor-specific antibody, a stable chemical linker (either cleavable or non-cleavable), and a potent cytotoxic payload with each playing a crucial role in determining the overall efficacy and safety of ADCs. Today, the success of ADCs could offer a much needed safer and more effective alternative to existing chemotherapy treatments.
Take Mirvetuximab Soravtansine (Elahere), for example. It was recently approved by the United States FDA as a first-in-class ADC used to treat adults with folate receptor-alpha (FRα)-positive, platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal cancer. Specifically, it targets FRα-expressing cells and releasing the cytotoxic anti-mitotic payload, DM4 to induce cell death. Following successful trials investigating its efficacy in the treatment of ovarian cancer,(3) one trial reported measurable tumor shrinkage in 44% of participants, and five individuals experienced complete responses to the novel treatment.(4)
However, as with many medical advances, translating that promise and expectation into measurable success in clinical trials is far from easy. The early promise of this new suite of cancer therapies must be tempered by the potential challenges involved in the study and delivery of the treatment.
Challenges in ADC development and clinical use
As researchers continue developing ADCs for ovarian and breast cancers, a few persistent challenges are proving difficult to ignore.
One of the main challenges researchers face is antigen downregulation. For example, the drug Trastuzumab Deruxtecan (T-DXd) has shown success in treating HER2 positive and HER2 low metastatic breast cancer, but in many cases, therapeutic resistance quickly builds as the HER2 expression is reduced or lost. This means that the ADC is unable to make contact with its target cells to release the drug.(5)
Then there is payload efflux, whereby the cytotoxic payload is actively pumped out by the cancerous cells so that the drug never reaches its target. This poses a further barrier in the trial stages.
Tumor heterogeneity adds another layer of complexity. Many tumors consist of a mix of different cell populations. As a result, while ADCs may effectively eliminate target cells, non-targeted bystander cells can remain unharmed, allowing the tumor to continue growing and spreading.
The composition of the tumor microenvironment itself also adds to some of the challenges. Components such as cancer-associated fibroblasts (CAFs) and the extracellular matrix (ECM) can obstruct ADC penetration, making it more difficult for the drug to reach and affect cancer cells deep within the tumor.
And of course, there are the practical challenges of running these studies. For one, immunohistochemistry (IHC) scoring, which is used to measure antigen levels, can vary from lab to lab, which makes it hard to get consistent results across different studies. Detecting small amounts of antigen also requires precision equipment that doesn’t come cheap or easily.
Then there’s the challenge of pharmacokinetic (PK) monitoring. You need to confirm that the ADC remains stable, the linker holds until precisely the right moment, and the payload is released on cue. Achieving this reliably across multiple global sites is nothing short of a logistical ballet.(6) It becomes especially critical in early-phase trials, when timing is tight and dose decisions need to be made at speed.
Future efforts focusing on overcoming resistance via combination strategies (by combining ADCs with immune checkpoint inhibitors [ICIs], PARP inhibitors, or other targeted agents), the use of novel targets, and bispecific ADCs are key to the development of the next-generation ADCs that aim to improve precision and efficacy. Indeed, what we’re witnessing is the field moving towards earlier lines of therapy (neoadjuvant/adjuvant) and using AI to personalize ADC selection, aiming for curative approaches rather than just progression delay.
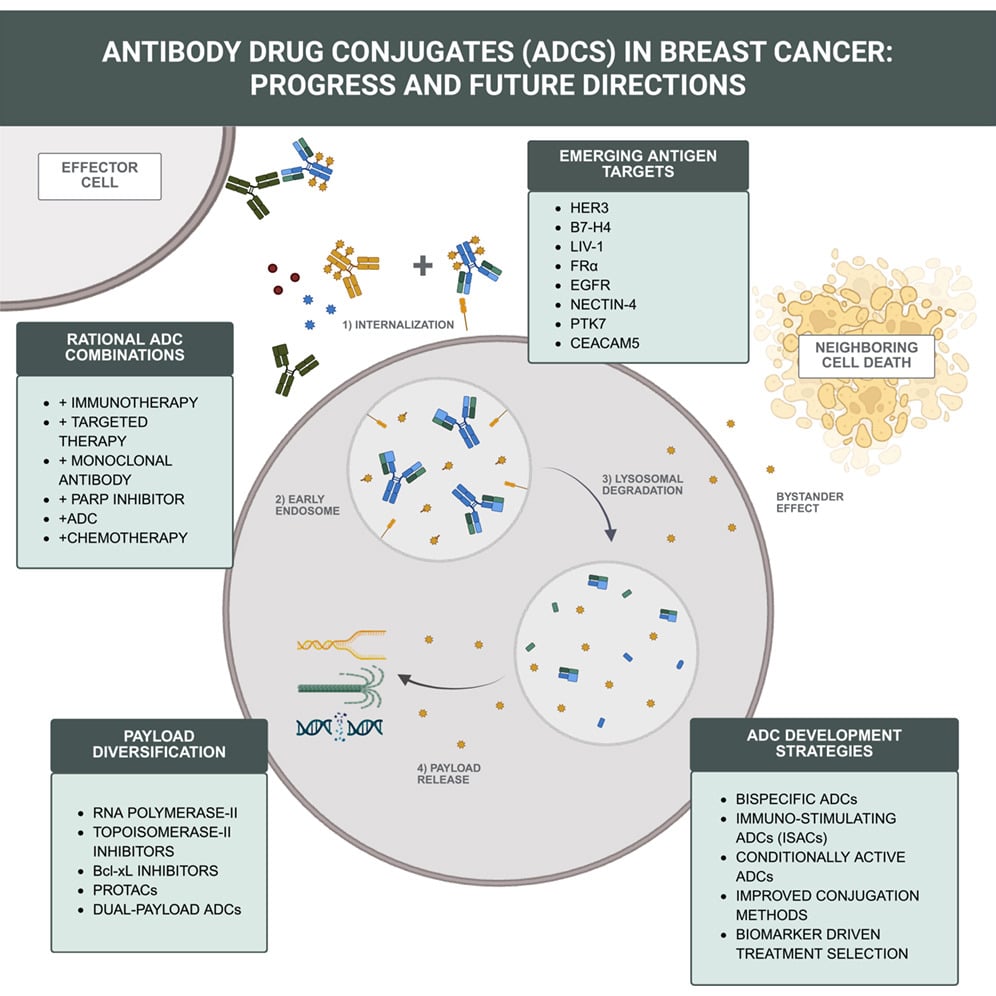
Figure 1: Newman et al., 2026: Antibody-drug conjugates in breast cancer: Progress and future directions.
Good practices and Cerba Research’s end-to-end support
Given how much is at stake, successfully running ADC trials demands precision, integration, and global coordination. For sponsors, even small mishaps during trial stages can lead to costly delays – which is why partnering with a lab that can manage the complexity at scale is absolutely essential.
Enter Cerba Research. Our end-to-end capabilities are designed to directly address the complex scientific, operational, and logistical challenges faced throughout all trial stages, significantly simplifying the process.
We can provide biomarker qualification using robust and reliable IHC, mIHC and ISH assays to test for expression of HER2, TROP2, FRα and NaPi2b.
Next-generation sequencing (NGS) is also available for monitoring the emergence of co-mutations e.g. the critical PIK3CA and ESR1 genes which, in hormone receptor-positive breast cancer, often drive therapy resistance and metastasis.
Our expert labs provide ligand-binding assays (LBA) that can accurately quantify ADC concentration in plasma, specifically the total antibody and conjugated antibody quantification. This is particularly important for ADCs carrying highly potent cytotoxic payloads.
Getting these measurements right is critical for balancing efficacy and safety, as well as the integrity of the study. It ensures that the drug is consistently reaching its target and that the payload is being released as intended. Reliable quantification also helps flag any issues with dosing or ADC stability early in the trial, potentially avoiding costly delays or adjustments later in the process.
Throughout the trial, patient safety remains our top priority. We provide comprehensive and compliant lab testing to monitor key indicators such as hematology and cytokine levels, particularly for immune-related adverse events (irAEs). Our safety monitoring ensures that any adverse reactions to treatments are closely monitored at all stages.
We also offer resistance monitoring using NGS to track emerging mutations and resistance mechanisms, as well as ctDNA analysis for non-invasive monitoring of tumor evolution. This means you can respond to emerging resistance throughout the study, enabling the identification of new and innovative strategies to overcome it.
On the logistical front, we handle the global coordination of FFPE and PBMC samples, managing collection, shipping, storage, and processing, all in line with global regulations. Our integrated, centralized model reduces dependence on multiple vendors, which in turn helps minimize the snags and delays that come from juggling too many moving parts.
Most importantly, it gives sponsors peace of mind that sample quality is protected, no matter how far those samples travel.
Peace of mind with support from a partner you can trust
We provide integrated, end-to-end support for ADC trials in ovarian and breast cancer. From safety testing and PK/PD analysis to in-depth biomarker work, our end-to-end service is designed to help you see the full picture: clear, precise, and just when you need it.
These studies can be complex. We take the operational weight off your shoulders so your team can focus on the science, not the logistics.
If you’re looking for a partner who understands the nuance and urgency of ADC development, and who’ll bring some calm to the chaos, we’re here for you. Let’s work together to move these promising therapies forward, and in doing so, bring better outcomes to people facing breast and ovarian cancer.
Key takeaways
- ADCs are reshaping cancer treatment: Targeted delivery of cytotoxic payloads offers improved efficacy and reduced systemic toxicity versus traditional chemotherapy.
- Resistance remains a key barrier: Antigen downregulation and payload efflux can limit ADC effectiveness and impact long-term outcomes.
- Tumor complexity affects response: Heterogeneity and microenvironment barriers can restrict ADC penetration and leave residual disease.
- Precision testing underpins success: Standardized IHC, sensitive detection methods, and robust PK monitoring are critical for reliable trial data.
- Integrated biomarker strategies enhance insight: Combining IHC, NGS, and ctDNA enables better patient stratification and real-time resistance monitoring.
- End-to-end support reduces risk: Centralized lab services and global sample management improve consistency, efficiency, and trial execution.